AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2641-8975/028
1 Department of Endocrinology, Army Hospital (R and R), New Delhi, India.
2Comd Hospital Lucknow
*Corresponding Author: Amit Nachankar, Department of Endocrinology, Army Hospital (R and R), New Delhi, India.
Citation: Amit Nachankar, Osteoporosis Prevalence and Correlates in Uncomplicated Type 2 Diabetes Mellitus. J. Diabetes and Islet Biology, 4(1); DOI:10.31579/2641-8975/028
Copyright: © 2021 Amit Nachankar, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 October 2021 | Accepted: 18 November 2021 | Published: 24 November 2021
Keywords: osteoporosis prevalence; type 2 diabetes mellitus; metabolic disorder
Type 2 Diabetes Mellitus (T2DM) is a common metabolic disorder at a pandemic proportion at present. Often T2DM is associated with microvascular (diabetic nephropathy, neuropathy, and retinopathy) and macrovascular complications (coronary artery disease, peripheral arterial disease, and stroke). Additionally diabetic osteopathy is a significant comorbidity of T2DM and is characterized by micro architectural changes that decrease bone quality leading to an increased risk of fragility fracture.
Introduction:
Type 2 Diabetes Mellitus (T2DM) is a common metabolic disorder at a pandemic proportion at present. Often T2DM is associated with microvascular (diabetic nephropathy, neuropathy, and retinopathy) and macrovascular complications (coronary artery disease, peripheral arterial disease, and stroke) [1]. Additionally diabetic osteopathy is a significant comorbidity of T2DM and is characterized by micro architectural changes that decrease bone quality leading to an increased risk of fragility fracture. [2]
Individuals with T2DM are often associated with a reduction of bone strength which might not be reflected in the measurement of bone mineral density (BMD). They show relatively reduced bone formation, osteoblast dysfunction, and low bone turnover. The low bone turnover has deleterious effects on bone health. Insulin deficiency decreases bone growth and turnover by decreased osteoblast recruitment. In advanced T2DM, insulin deficiency could impair bone homeostasis through dysregulation of the growth hormone-IGF-1 axis. Pooled data has shown that bone turnover markers (BTM) such as osteocalcin, procollagen type 1 amino terminal pro-peptide and bone resorption markers such as C-terminal cross-linked telopeptide were significantly lower among those with T2DM and did not necessarily correlate with glucose level. So T2DM should be considered a state of low bone turnover, perhaps driven by increased serum levels of sclerostin and osteoprotegerin which inhibit osteoblast and osteoclast differentiation respectively.
Strotmeyer et al [3] have shown increased BMD in T2DM due to associated obesity but also increased risk of fragility fractures due to altered bone microarchitecture. Dutta et al [4] have showed decreased BMD in T2DM. Some studies have shown association of poor glycemic control with increased osteoporosis and fragility fractures whereas others have shown no effect of glycemic control on fragility fractures in T2DM. Many studies have shown osteopenic effects of certain antidiabetic drugs (thiazolidinediones, SGLT 2 inhibitors and insulin) on increased fragility fracture prevalence in T2DM. Hence, the present study was conducted with the aim to evaluate the prevalence of osteoporosis in T2DM using the BMD by dual Xray absorptiometry (DXA) and its correlation with various factors in uncomplicated T2DM population.
This cross-sectional observational study was conducted at a multidisciplinary tertiary care hospital in North India involving 100 T2DM patients attending medicine/endocrinology outpatient department. They were enrolled during the study period of 1.5 year (From Mar 2019 to Sep 2020). The inclusion criteria was T2DM patients of age 50 years and above, either gender, new or known T2DM. The exclusion criteria were: Patients diagnosed with diabetes-associated microvascular and macrovascular complications, chronic smokers, chronic kidney disease, thyroid/parathyroid disorders, obvious bone and mineral disorders, chronic pancreatitis or postpancreatectomy, systemic inflammatory disorders, malabsorption syndromes, malignancy, or those receiving corticosteroids, immunosuppressants, anticonvulsants, thiazolidinediones or insulin; chronic debility or bedridden patients and those unwilling to participate in study.
After ethical approval and written consent of the patients, all the patients falling in sampling frame were enrolled. Demographic information was obtained from all the patients. Clinical history, duration of diabetes, treatment history and current medication profile was noted. All underwent anthropometric assessment and body mass index (BMI) was calculated. A detailed clinical examination was carried out. Blood samples were collected in fasting and 2hour post prandial from all the patients and were analyzed for fasting blood glucose (FBG) & post prandial blood glucose (PPBG), HbA1c, serum calcium, phosphorus, total protein, albumin and Vitamin D levels. All the patients underwent BMD-DXA evaluation by Hologic machine at two sites – spine and hip. For each site, calibration was performed before scans in every patient. Proper positioning was ascertained before and during the scans. The same trained technician performed DXA scans in all patients. T-scores were calculated. As recommended by the World Health Organization a T-score of 2.5 or lower was considered as osteoporosis at either site while T-score between −1.0 and −2.4 was considered as osteopenia. Data was collected on a proforma and was later entered into computer using Microsoft Excel software.
Statistical Methods:
Data was analyzed using Statistical Package for Social Sciences, version 21.0. Qualitative data has been represented as numbers and percentages while quantitative/ continuous data has been represented as mean±standard deviation. Analysis of variance and chi-square test were used to compare the data. A ‘p’ value less than 0.05 was considered as statistically significant.
The baseline profile of the subjects in the study is as in table 1.

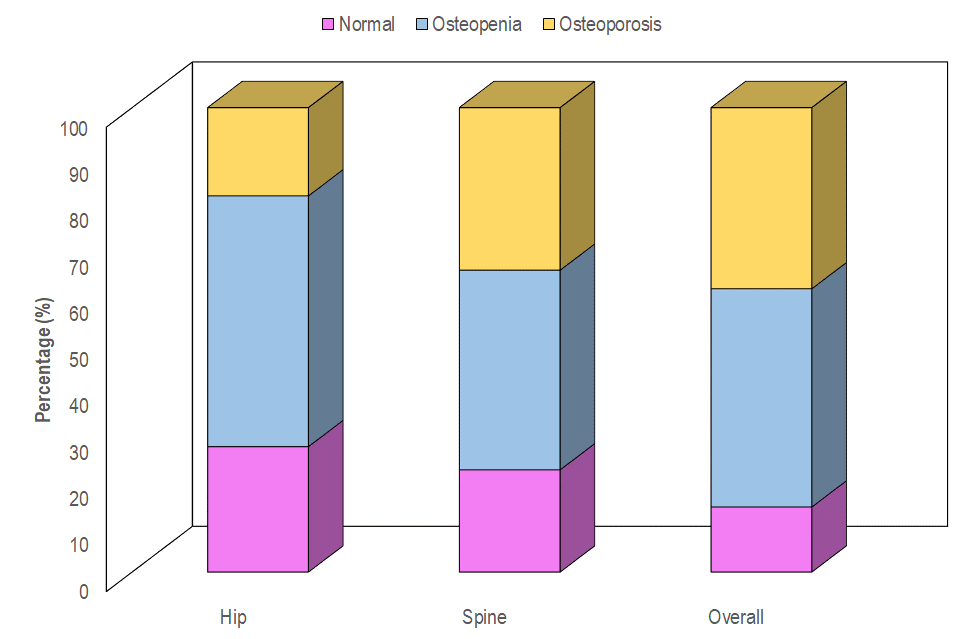
The age of patients ranged from 50-80 years, with a mean age of 59.39±7.01 years. The mean BMI of patients was 25.94±9.97 kg/m2 and the BMI ranged from 16.44-34.02 kg/m2. There were 40% overweight and 16% obese patients with 2% underweight. The duration of T2DM ranged from 1 to 15 years with mean of 6.21±2.56 years. All were taking metformin for glycaemia control and a majority (75.0%) of them were also taking Sulfonylureas. Only a few (28.0%) were taking DPP4 inhibitors. The only comorbidity of primary hypertension was present in 23(23.0%) patients. The average fasting glucose of 132 mg/dl and postprandial glucose was 182mg/dl in the study population with average HbA1c 7.7%. Distribution of Study Population according to BMD at different sites is shown in figure 1. Overall 47% patients had Osteopenia and 39% had Osteoporosis. At Lumbar Spine, 43% patients had osteopenia and 35% had osteoporosis. Similarly at Hip, 54.0% had Osteopenia and only 19% had osteoporosis.
For BMD findings, mean age of patients with osteoporosis (61.26±6.92 years) was higher as compared to cases with osteopenia (59.15±7.20 years) or normal BMD (55.0±4.42 years) and this difference was statistically significant (p=0.014). A higher proportion of females had osteopenia (68.1%) and osteoporosis (84.6%) as compared to males (osteopenia:31.9%; osteoporosis:15.4%) and this difference was statistically significant (p<0 p=0.301).>
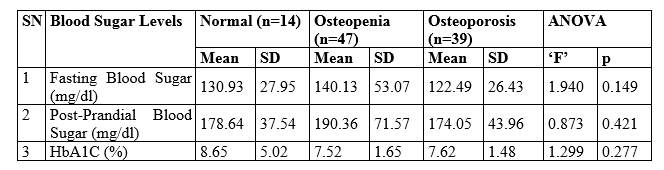
The mean FBG in osteoporosis patient (122.49±26.43mg/dl ) was lower than in osteopenia (140.13±53.07mg/dl) or normal BMD (130.93±27.95mg/dl). The mean PPBG in osteoporosis patient (174.05±43.96mg/dl ) was lower than in osteopenia (190.36±71.57mg/dl) or normal BMD (178.64±37.54mg/dl). The mean HbA1c in osteoporosis patients (7.62±1.48%) was lower than in normal BMD (7.52±5.02%) with osteopenia patients had HbA1c of 7.52±1.65%. None of these showed any significant difference as in Table 2.
Normal BMD cases had a higher mean vitamin-D levels (32.68±17.90 ng/ml) as compared to osteopenia cases (29.20±13.27 ng/ml) or osteoporosis cases (22.64±15.52 ng/ml). (Table 3) This difference was found to be statistically significant (p=0.044). However, no significant association between severity of osteoporosis with calcium levels was found (p=0.226). Conversely majority (46.2%) of osteoporosis cases had Vitamin-D deficiency, followed by insufficient Vitamin-D in 35.9%. Only very few (17.9%) osteoporosis cases had normal

Vitamin D levels. However, higher proportions of osteopenia (48.9%) and normal BMD cases (57.1%) had normal vitamin D levels. Further, only 3 (21.4%) normal BMD cases had vitamin D deficiency or insufficiency. Similarly 12 (25.5%) osteopenia cases had vitamin D deficiency or insufficiency. This difference was statistically significant (p=0.044).
A majority (46.2%) of osteoporosis cases had Vitamin-D deficiency, followed by insufficiency (35.9%). Only 20% osteoporosis cases had normal vitamin D. However in osteopenia cases, higher proportions (48.9%) had normal vitamin D, followed by 25.6
Our study had a mean age of 59.39±7.01 years similar to Agrawal and Sharma [5] whose study on 200 males aged 50 years or more reported mean age of 62.61±7.64 years. A cross-sectional study by Sharma et al. [6] evaluated osteoporosis in 200 T2DM patients and reported a mean age of 64.5±7.0 years. Similar study by Asokan et al. [7] had mean age 56years in T2DM patients. Our study has 39% prevalence of osteoporosis (with 47% osteopenia) thereby showing highly compromised BMD in T2DM. Compromised BMD has been reported to be quite high among T2DM in different studies from across different parts of India. Table 4 shows the profile of some of the contemporary studies from India studying the prevalence of osteopenia and osteoporosis in T2DM and compares them with our study. Low prevalence rate of
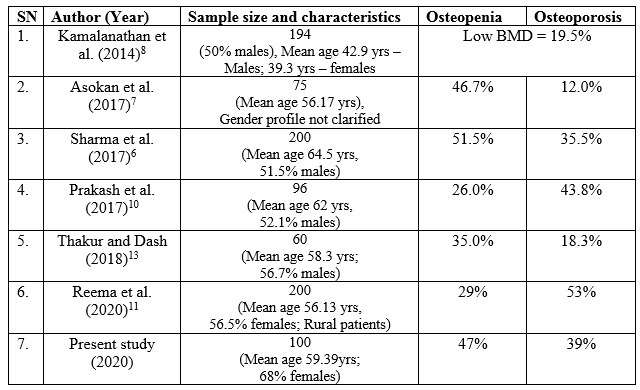
low BMD (19.5%) in the study of Kamalanathan et al. [8] could be primarily due to much younger patients (mean age 42.9 years for males and 39.3 years for females) as compared to other studies showing mean age 55-65 years at increased risk of osteoporosis.[9] However, most of the previous studies show a high prevalence of osteopenia and osteoporosis in T2DM.
Our study had relatively more osteopenia (47%) patients than osteoporosis (39%) which is in agreement with the observation of Sharma et al.6 who also had higher number of osteopenia (51.5%) patients than osteoporosis (35.5%). They had an overall prevalence of osteopenia and osteoporosis close to ours (87% vs 86% in our study). Though Prakash et al.[10] also reported the prevalence of osteopenia and osteoporosis to be quite high (69.8%), however, in their study the prevalence of osteoporosis was higher (43.8%) as compared to osteopenia (26%). Reema et al.11 reported the overall prevalence of osteopenia and osteoporosis to be close to our study (82% vs 86% in our study), yet in their study proportion of osteoporosis was much higher (53%) than our study (39%) whereas proportion of those with osteopenia was much lower (29%) than our study (47%). These finding suggest that although, there is a high prevalence of osteopenia and osteoporosis in T2DM patients yet the pattern and spectrum of these BMD abnormalities shows a considerable variance. These findings imply that apart from T2DM other factors also play a role in BMD.
In our study, the osteoporosis prevalence at Lumbar spine (35%) was higher than at hip (19%). These findings are in agreement with the observations of Prakash et al. [10] who also found both prevalence of osteoporosis to be higher at Lumbar spine (39.6%) as compared to hip (20.8%). Sharma et al. [6] also observed that prevalence of osteoporosis at spine was 33.5% whereas at hip it was 13.5%. A similar observation was also made by Kamalnathan et al.[8] who reported mean Z-scores for BMD at spine to be lower as compared to that at hip. However, LeidigBruckner et al.12 reported the greater prevalence of osteoporosis at hip (13% men and 21.9% women) than at spine (6.1% men and 9.4% women). The difference could probably be owing to difference in occupation and lifestyle pattern of Asians as compared to western population.
Our study did not find a significant association of BMD with glycemic status i.e. FBG and PPBG levels or HbA1c. Association of BMD with glycemic status are controversial. In a recent report Thakur and Dash [13] found mean HbA1c of patients with low BMD to be significantly lower as compared to those having high BMD, thus showing good glycemic control to be associated with an increased risk of BMD loss. Conversely, they observed mean FBG of those with low BMD to be higher as compared to those having high BMD, thus painting just a reverse picture as observed for HbA1c. Mobini et al.[14] in a study among T2DM women also found comparable HbA1c levels between women with and without osteoporosis. Dutta et al. [4] also did not find a significant association between BMD and HbA1c levels. In fact, the observation made by Kamalanathan et al.[8] ruled out any effect of glycemic status on BMD who in a case-control study did not find a significant difference in BMD of Indian T2DM patients as compared to healthy volunteers. Asokan et al.[7] also did not find a significant difference in BMD of T2DM cases as compared to controls, and thus ruled out an association of level of glycemic control with BMD. In our study, the non-existence of a relationship between level of glycemic control and BMD also showed that hyperglycemia per se cannot be the sole factor being responsible for BMD loss in T2DM.
In our study, age was found to be significantly associated with severity of osteoporosis. Moreover, the increased loss of BMD was observed with increasing age. These findings confirm that age continues to be one of the deterministic factors in BMD loss in T2DM as well. The relationship between age and BMD loss is governed by two factors. First, with advancing age there is an imbalance between resorption and formation (resorption higher than formation), thereby increased BMD loss. Secondly, increasing age results in degenerative changes thereby decreasing physical activity [9]. Reema et al.[11] in their study observed increasing age to be associated with increased odds of BMD loss in both univariate as well as multivariate analysis. Prakash et al.[10] also observed a positive correlation between BMD loss with advancing age. As such, the association between advancing age and BMD loss is a universal phenomenon seen in all the populations irrespective of T2DM status [15,16,17].
Our study did not find a significant association of waist circumference or BMI with BMD loss. Our observations are in contradiction with the observations of Leidig-Bruckner et al. [12] and Oei et al. [18] where BMD was positively correlated with BMI. Reema et al.[11] and Prakash et al. [10]also found a protective effect of increased BMI against BMD loss. However, in our study, no such protective effect of BMI could be seen.
We also could not find a significant association between duration of diabetes and BMD status. However, a number of studies found duration of diabetes to be significantly associated with BMD loss [10,11,13,19]. One of the reasons could be primarily the present study had only few cases with T2DM duration >10 years (mean duration of T2DM 6.21 years). Compared to our study, Prakash et al.[6,5] had 35.4% patients with T2DM duration >10 years and also included patients with T2DM duration >15 years. Our study findings are in agreement with the observations of Mobini et al.[14] who also did not find a significant association between osteoporosis and duration of diabetes. The relationship between duration of T2DM and BMD loss is often confounded with ageing. In the studies having a higher mean age of patients, the T2DM duration often coincide with the increasing age. Relatively low mean age of patients in our study could be another factor responsible for non-existence of a relationship between duration of T2DM and BMD. In a recent study, Jang et al.[20] also found that T2DM males having duration of T2DM >5 years had low BMD as compared to those having T2DM duration <5>5 years were significantly older in age as compared to those having duration of diabetes <5>
In our study, females had a significant association with BMD loss in T2DM. female sex in postmenopausal age group are a known risk group for osteoporosis due to significantly increased bone resorption over formation due to low levels of estrogen thus inducing accelerated bone loss [15]. Similar to our observations, Sharma et al.[6] also found BMD to be lower in females as compared to males. Studies by other workers also supported this observation [10,11].
Our study found vitamin D levels to be positively associated with BMD. There was a significant decreasing trend of mean vitamin D levels with increasing severity of BMD loss. Prevalence of vitamin D insufficiency and deficiency was also significantly higher in osteopenia and osteoporosis as compared to those with normal BMD. However, no such association was seen with serum calcium levels. The role of vitamin D in calcium resorption and bone formation is well-documented as calcium is an essential ingredient of bone. However, the association of vitamin D level and calcium with BMD in T2DM has been documented to be of differential nature in different studies. Sharma et al.[6] in their study did not find a significant correlation of both calcium and vitamin D levels with BMD. Reema et al.[11] in their study found low calcium levels to be significantly associated with BMD loss, however, they did not study the association of vitamin D levels with BMD. Kamalanathan et al.[8] in contrast did not find a significant association of either calcium or vitamin D levels with BMD loss. Agarwal et al.[5]found low vitamin D levels to be significantly associated with an increased risk of osteopenia and osteoporosis but did not report any such association with serum calcium.
One of the limitations of present study was lack of a control group owing to which it is difficult to say whether the prevalence of osteopenia and osteoporosis is affected by T2DM status and whether the factors governing BMD loss in T2DM are different from non-diabetic individuals. Hence, further studies on a larger population with inclusion of a non-diabetic control population are recommended to understand these issues further. Secondly, we did not assess parathyroid or testosterone levels thereby missing on normocalcemic hyperparathyroidism or hypogonadism in males. Also we did not record menopausal status in female T2DM patients thereby missing in some obvious postmenopausal osteoporosis. Thirdly latest innovations in BMD include trabecular bone score(TBS) software which detects qualitative assessment of degradation of bone microarchitecture. Addition of TBS score would have helped assess T2DM patient with normal BMD who are having partially or severely degraded bone architecture. Fourthly, BTM assessment could have helped to identify role of T2DM in low BMD states.
Our study had 39% osteoporosis prevalence in T2DM (Hip:19.0%; Spine:35.0%) in addition to 47% osteopenia (Hip:54.0%; Spine:43.0%). No significant association of osteoporosis was noted with BMI, waist circumference, duration of T2DM or glycemic status. But significant association of osteoporosis was with age & female gender. Additionally, significant association of osteoporosis was observed with vitamin D deficiency or insufficiency but not with serum calcium. Prevalence of lumbar spine osteoporosis was more than hip osteoporosis but no differences among risk factors associated with overall osteoporosis as compared to lumbar spine or hip osteoporosis seperately.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
